
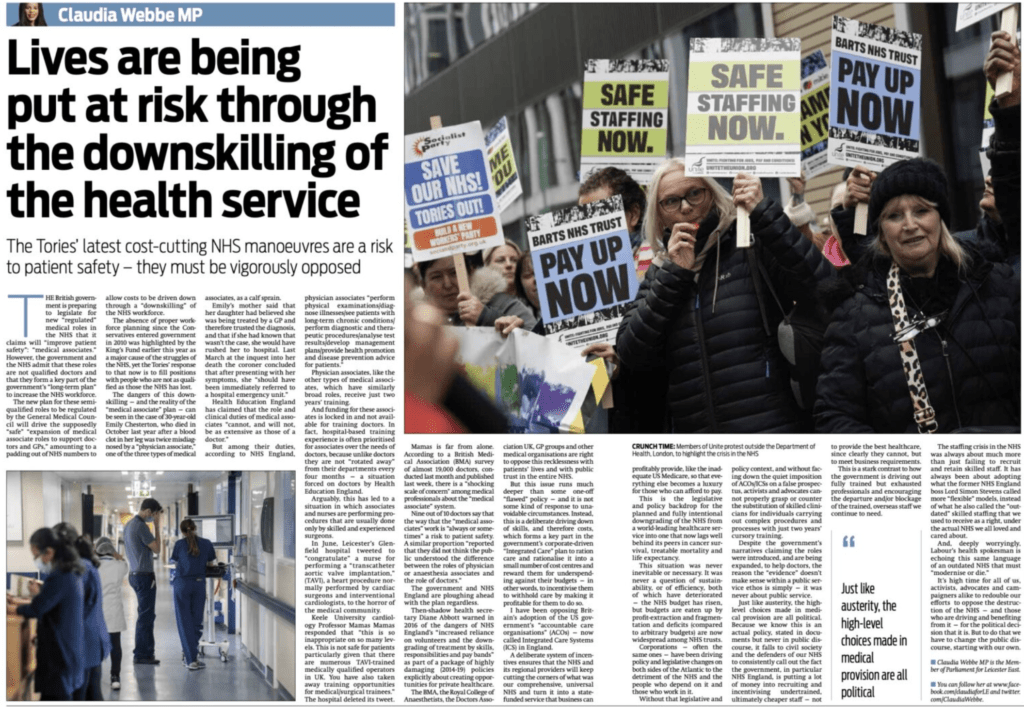
Lives are being put at risk through the downskilling of the NHS
By Claudia Webbe MP
The government’s latest cost-cutting NHS manoeuvres are a risk to patient safety – they must be vigorously opposed, warns CLAUDIA WEBBE MP
THE British government is preparing to legislate for new “regulated” medical roles in the NHS that it claims will “improve patient safety”: “medical associates.” However, the government and the NHS admit that these roles are not qualified doctors and that they form a key part of the government’s “long-term plan” to increase the NHS workforce.
The new plan for these semi-qualified roles to be regulated by the General Medical Council will drive the supposedly “safe” “expansion of medical associate roles to support doctors and GPs,” amounting to a padding out of NHS numbers to allow costs to be driven down through a “downskilling” of the NHS workforce.
The absence of proper workforce planning since the Conservatives entered government in 2010 was highlighted by the King’s Fund earlier this year as a major cause of the struggles of the NHS, yet the Tories’ response to that now is to fill positions with people who are not as qualified as those the NHS has lost.
The dangers of this downskilling — and the reality of the “medical associate” plan — can be seen in the case of 30-year-old Emily Chesterton, who died in October last year after a blood clot in her leg was twice misdiagnosed by a “physician associate,” one of the three types of medical associates, as a calf sprain.
Emily’s mother said that her daughter had believed she was being treated by a GP and therefore trusted the diagnosis, and that if she had known that wasn’t the case, she would have rushed her to hospital. Last March at the inquest into her death the coroner concluded that after presenting with her symptoms, she “should have been immediately referred to a hospital emergency unit.”
Health Education England has claimed that the role and clinical duties of medical associates “cannot, and will not, be as extensive as those of a doctor.”
But among their duties, according to NHS England, physician associates “perform physical examinations/diagnose illnesses/see patients with long-term chronic conditions/perform diagnostic and therapeutic procedures/analyse test results/develop management plans/provide health promotion and disease prevention advice for patients.”
Physician associates, like the other types of medical associates, which have similarly broad roles, receive just two years’ training.
And funding for these associates is locked in and not available for training doctors. In fact, hospital-based training experience is often prioritised for associates over the needs of doctors, because unlike doctors they are not “rotated away” from their departments every four months — a situation forced on doctors by Health Education England.
Arguably, this has led to a situation in which associates and nurses are performing procedures that are usually done only by skilled and experienced surgeons.
In June, Leicester’s Glenfield hospital tweeted to “congratulate” a nurse for performing a “transcatheter aortic valve implantation,” (TAVI), a heart procedure normally performed by cardiac surgeons and interventional cardiologists, to the horror of the medical community.
Keele University cardiology Professor Mamas Mamas responded that “this is so inappropriate on so many levels. This is not safe for patients particularly given that there are numerous TAVI-trained medically qualified operators in UK. You have also taken away training opportunities for medical/surgical trainees.” The hospital deleted its tweet.
Mamas is far from alone. According to a British Medical Association (BMA) survey of almost 19,000 doctors, conducted last month and published last week, there is a “shocking scale of concern” among medical professionals about the “medical associate” system.
Nine out of 10 doctors say that the way that the “medical associates” work is “always or sometimes” a risk to patient safety. A similar proportion “reported that they did not think the public understood the difference between the roles of physician or anaesthesia associates and the role of doctors.”
The government and NHS England are ploughing ahead with the plan regardless.
Then-shadow health secretary Diane Abbott warned in 2016 of the dangers of NHS England’s “increased reliance on volunteers and the downgrading of treatment by skills, responsibilities and pay bands” as part of a package of highly damaging (2014-19) policies explicitly about creating opportunities for private healthcare.
The BMA, the Royal College of Anaesthetists, the Doctors Association UK, GP groups and other medical organisations are right to oppose this recklessness with patients’ lives and with public trust in the entire NHS.
But this issue runs much deeper than some one-off “flawed” policy — and it is not some kind of response to unavoidable circumstances. Instead, this is a deliberate driving down of skills, and therefore costs, which forms a key part in the government’s corporate-driven “Integrated Care” plan to ration care and rationalise it into a small number of cost centres and reward them for underspending against their budgets — in other words, to incentivise them to withhold care by making it profitable for them to do so.
I have been opposing Britain’s adoption of the US government’s “accountable care organisations” (ACOs) — now called Integrated Care Systems (ICS) in England.
A deliberate system of incentives ensures that the NHS and its regional providers will keep cutting the corners of what was our comprehensive, universal NHS and turn it into a state-funded service that business can profitably provide, like the inadequate US Medicare, so that everything else becomes a luxury for those who can afford to pay.
This is the legislative and policy backdrop for the planned and fully intentional downgrading of the NHS from a world-leading healthcare service into one that now lags well behind its peers in cancer survival, treatable mortality and life expectancy.
This situation was never inevitable or necessary. It was never a question of sustainability, or of efficiency, both of which have deteriorated — the NHS budget has risen, but budgets are eaten up by profit-extraction and fragmentation and deficits (compared to arbitrary budgets) are now widespread among NHS trusts.
Corporations — often the same ones — have been driving policy and legislative changes on both sides of the Atlantic to the detriment of the NHS and the people who depend on it and those who work in it.
Without that legislative and policy context, and without facing down the quiet imposition of ACOs/ICSs on a false prospectus, activists and advocates cannot properly grasp or counter the substitution of skilled clinicians for individuals carrying out complex procedures and processes with just two years’ cursory training.
Despite the government’s narratives claiming the roles were introduced, and are being expanded, to help doctors, the reason the “evidence” doesn’t make sense within a public service ethos is simply — it was never about public service.
Just like austerity, the high-level choices made in medical provision are all political. Because we know this is an actual policy, stated in documents but never in public discourse, it falls to civil society and the defenders of our NHS to consistently call out the fact the government, in particular NHS England, is putting a lot of money into recruiting and incentivising undertrained, ultimately cheaper staff — not to provide the best healthcare, since clearly they cannot, but to meet business requirements.
This is a stark contrast to how the government is driving out fully trained but exhausted professionals and encouraging the departure and/or blockage of the trained, overseas staff we continue to need.
The staffing crisis in the NHS was always about much more than just failing to recruit and retain skilled staff. It has always been about adopting what the former NHS England boss Lord Simon Stevens called more “flexible” models, instead of what he also called the “outdated” skilled staffing that we used to receive as a right, under the actual NHS we all loved and cared about.
And, deeply worryingly, Labour’s health spokesman is echoing this same language of an outdated NHS that must “modernise or die.”
It’s high time for all of us, activists, advocates and campaigners alike to redouble our efforts to oppose the destruction of the NHS — and those who are driving and benefiting from it — for the political decision that it is. But to do that we have to change the public discourse, starting with our own.
Claudia Webbe MP is the member of Parliament for Leicester East. You can follow her at www.facebook.com/claudiaforLE and twitter.com/ClaudiaWebbe