
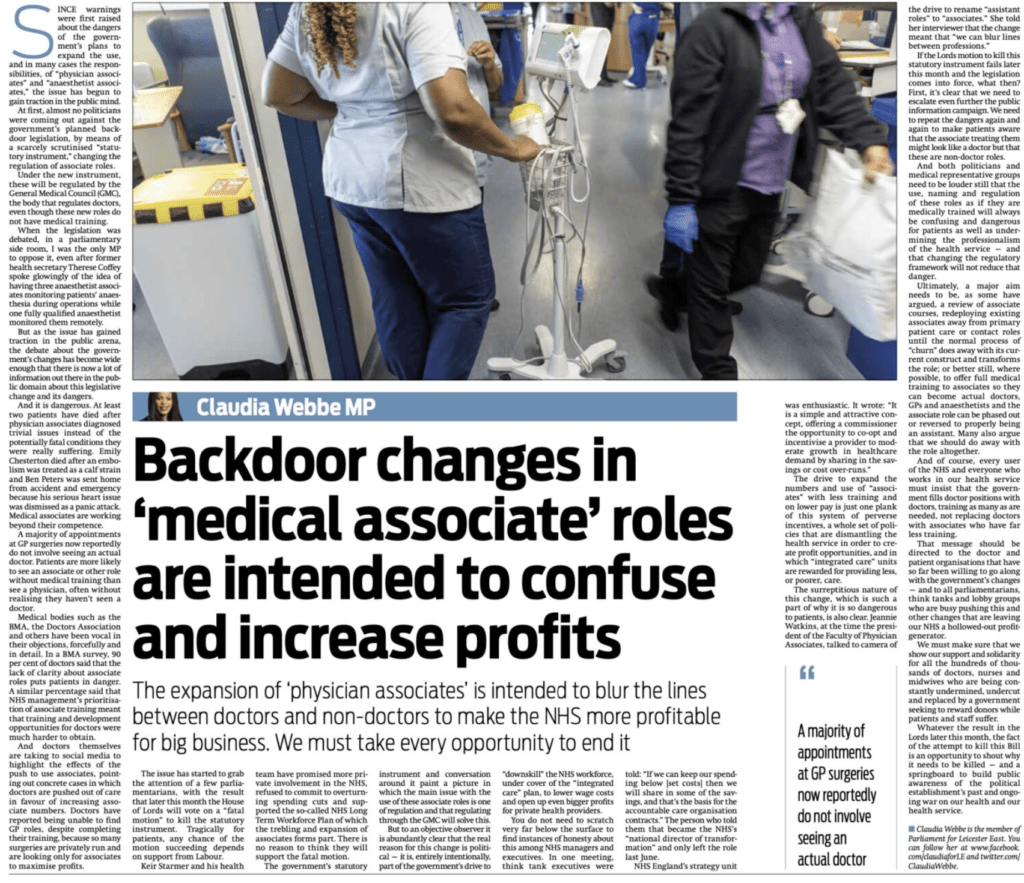
The backdoor changes in ‘medical associate’ roles are intended to confuse and increase profits
By Claudia Webbe MP
The expansion of ‘physician associates’ is intended to blur the lines between doctors and non-doctors to make the NHS more profitable for big business. We must take every opportunity to end it, says CLAUDIA WEBBE MP
SINCE warnings were first raised about the dangers of the government’s plans to expand the use, and in many cases the responsibilities, of “physician associates” and “anaesthetist associates,” the issue has begun to gain traction in the public mind.
At first, almost no politicians were coming out against the government’s planned backdoor legislation, by means of a scarcely scrutinised “statutory instrument,” changing the regulation of associate roles.
Under the new instrument, these will be regulated by the General Medical Council (GMC), the body that regulates doctors, even though these new roles do not have medical training.
When the legislation was debated, in a parliamentary side room, I was the only MP to oppose it, even after former health secretary Therese Coffey spoke glowingly of the idea of having three anaesthetist associates monitoring patients’ anaesthesia during operations while one fully qualified anaesthetist monitored them remotely.
But as the issue has gained traction in the public arena, the debate about the government’s changes has become wide enough that there is now a lot of information out there in the public domain about this legislative change and its dangers.
And it is dangerous. At least two patients have died after physician associates diagnosed trivial issues instead of the potentially fatal conditions they were really suffering. Emily Chesterton died after an embolism was treated as a calf strain and Ben Peters was sent home from accident and emergency because his serious heart issue was dismissed as a panic attack. Medical associates are working beyond their competence.
A majority of appointments at GP surgeries now reportedly do not involve seeing an actual doctor. Patients are more likely to see an associate or other role without medical training than see a physician, often without realising they haven’t seen a doctor.
Medical bodies such as the BMA, the Doctors Association and others have been vocal in their objections, forcefully and in detail. In a BMA survey, 90 per cent of doctors said that the lack of clarity about associate roles puts patients in danger. A similar percentage said that NHS management’s prioritisation of associate training meant that training and development opportunities for doctors were much harder to obtain.
And doctors themselves are taking to social media to highlight the effects of the push to use associates, pointing out concrete cases in which doctors are pushed out of care in favour of increasing associate numbers. Doctors have reported being unable to find GP roles, despite completing their training, because so many surgeries are privately run and are looking only for associates to maximise profits.
The issue has started to grab the attention of a few parliamentarians, with the result that later this month the House of Lords will vote on a “fatal motion” to kill the statutory instrument. Tragically for patients, any chance of the motion succeeding depends on support from Labour.
Keir Starmer and his health team have promised more private involvement in the NHS, refused to commit to overturning spending cuts and supported the so-called NHS Long Term Workforce Plan of which the trebling and expansion of associates forms part. There is no reason to think they will support the fatal motion.
The government’s statutory instrument and conversation around it paint a picture in which the main issue with the use of these associate roles is one of regulation and that regulating through the GMC will solve this.
But to an objective observer it is abundantly clear that the real reason for this change is political — it is, entirely intentionally, part of the government’s drive to “downskill” the NHS workforce, under cover of the “integrated care” plan, to lower wage costs and open up even bigger profits for private health providers.
You do not need to scratch very far below the surface to find instances of honesty about this among NHS managers and executives. In one meeting, think tank executives were told: “If we can keep our spending below [set costs] then we will share in some of the savings, and that’s the basis for the accountable care organisation contracts.” The person who told them that became the NHS’s “national director of transformation” and only left the role last June.
NHS England’s strategy unit was enthusiastic. It wrote: “It is a simple and attractive concept, offering a commissioner the opportunity to co-opt and incentivise a provider to moderate growth in healthcare demand by sharing in the savings or cost over-runs.”
The drive to expand the numbers and use of “associates” with less training and on lower pay is just one plank of this system of perverse incentives, a whole set of policies that are dismantling the health service in order to create profit opportunities, and in which “integrated care” units are rewarded for providing less, or poorer, care.
The surreptitious nature of this change, which is such a part of why it is so dangerous to patients, is also clear. Jeannie Watkins, at the time the president of the Faculty of Physician Associates, talked to camera of the drive to rename “assistant roles” to “associates.” She told her interviewer that the change meant that “we can blur lines between professions.”
If the Lords motion to kill this statutory instrument fails later this month and the legislation comes into force, what then? First, it’s clear that we need to escalate even further the public information campaign. We need to repeat the dangers again and again to make patients aware that the associate treating them might look like a doctor but that these are non-doctor roles.
And both politicians and medical representative groups need to be louder still that the use, naming and regulation of these roles as if they are medically trained will always be confusing and dangerous for patients as well as undermining the professionalism of the health service — and that changing the regulatory framework will not reduce that danger.
Ultimately, a major aim needs to be, as some have argued, a review of associate courses, redeploying existing associates away from primary patient care or contact roles until the normal process of “churn” does away with its current construct and transforms the role; or better still, where possible, to offer full medical training to associates so they can become actual doctors, GPs and anaesthetists and the associate role can be phased out or reversed to properly being an assistant. Many also argue that we should do away with the role altogether.
And of course, every user of the NHS and everyone who works in our health service must insist that the government fills doctor positions with doctors, training as many as are needed, not replacing doctors with associates who have far less training.
That message should be directed to the doctor and patient organisations that have so far been willing to go along with the government’s changes — and to all parliamentarians, think tanks and lobby groups who are busy pushing this and other changes that are leaving our NHS a hollowed-out profit-generator.
We must make sure that we show our support and solidarity for all the hundreds of thousands of doctors, nurses and midwives who are being constantly undermined, undercut and replaced by a government seeking to reward donors while patients and staff suffer.
Whatever the result in the Lords later this month, the fact of the attempt to kill this Bill is an opportunity to shout why it needs to be killed — and a springboard to build public awareness of the political establishment’s past and ongoing war on our health and our health service.
Claudia Webbe MP is the member of Parliament for Leicester East. You can follow her at www.facebook.com/claudiaforLE and twitter.com/ClaudiaWebbe